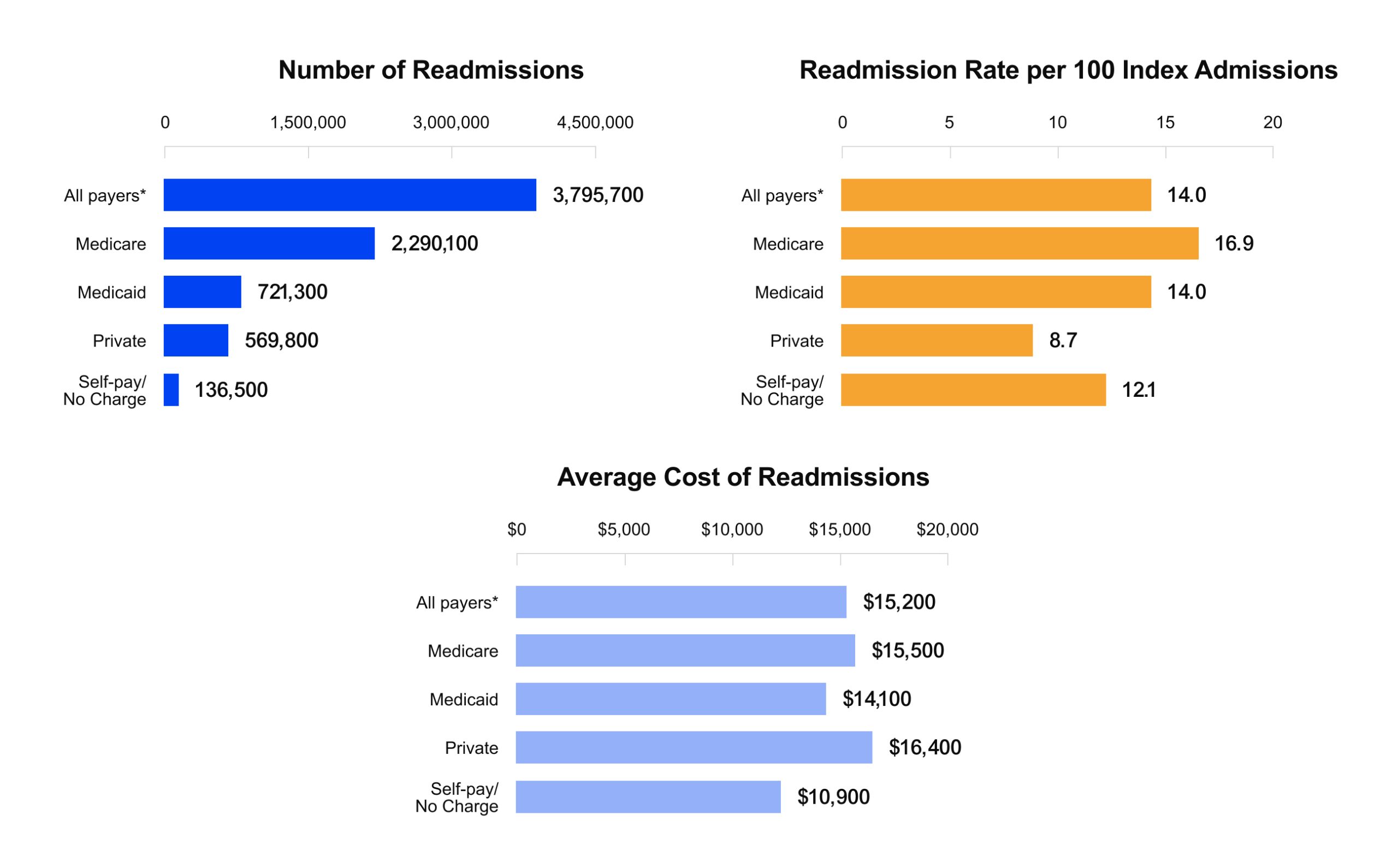
Chronic disease detection is hard to do well, and when it slips, chronic disease management becomes more expensive and less predictable. The impact shows up in avoidable utilization and financial volatility. In the U.S., there were 3.8 million adult 30-day readmissions, with an average cost of $15,200 per readmission. Hospitals also face direct reimbursement exposure through the Hospital Readmissions Reduction Program (HRRP), where payment reductions can reach up to 3%.
Healthcare organizations use various tools and methods to detect chronic diseases within broader disease and chronic condition management programs, including registries, rules, risk scores, and clinician review. Analytics that reconstruct longitudinal history and surface multi-factor patterns help teams detect chronic trajectories earlier and more consistently. Kodjin Analytics is a clinical analytics software designed for this approach. It turns longitudinal clinical and financial signals into explainable chronic cohorts, supports advanced cohort building, and helps leaders answer many day-to-day questions without SQL bottlenecks.
This article explains what chronic disease management is in practical terms and why detection quality is the foundation for chronic care management (CCM) execution in healthcare programs. It covers what high-quality detection means beyond diagnosis codes, what conditions qualify for chronic care management, and how the value differs for hospitals, clinics, and integrated delivery systems. It also shows how Kodjin supports can turn cohorts into practical worklists and interventions.
Highlights:
- HRRP creates direct financial exposure, with payment reductions that can reach up to 3% when readmissions stay high.
- Missed chronic patterns also increase preventable inpatient load, with 12.9% of adult nonobstetric stays reported as potentially preventable in one national analysis.
- Strong chronic disease management and CCM in healthcare depend on longitudinal, multi-criteria cohorts that stay consistent across teams, stages, and care settings.
- Kodjin Analytics turns clinical and financial history into explainable cohorts and worklists, so leaders can move faster from cohort definition to measurable interventions and outcomes.
Why High-Quality Chronic Disease Detection Matters
High-quality chronic disease detection is strategic because it decides who enters your “chronic care system” in the first place. For example, a diabetes detection cohort can include patients who missed an HbA1c test within the expected monitoring window, plus patients with highly variable point-in-time glucose results who also show supporting longitudinal signals, such as repeat abnormal readings, medication history consistent with diabetes management, and related comorbidity patterns. This kind of multi-criteria cohort is actionable because it produces a clear outreach worklist and a consistent follow-up protocol.
If the organization cannot identify chronic patients early and consistently, even the best care programs become reactive. Teams intervene after deterioration, and they often focus on the wrong patients because the definition of “chronic” shifts across departments and settings.
Chronic disease sits at the center of healthcare cost and utilization, so weak identification quickly becomes a financial problem. In the U.S., 90% of annual health care expenditures are for people with chronic and mental health conditions, which means small detection errors can scale into a large budget impact.
When chronic status is unclear in day-to-day workflows, patients reenter the system through recurring ED visits, repeat admissions, escalating medication regimens, and fragmented follow-up. This pattern also shows up in system-level utilization signals: AHRQ reported that about 12.9% of adult nonobstetric inpatient stays were potentially preventable, and most involved chronic care conditions that could be better managed with stronger outpatient and longitudinal control. Even strong cohort logic fails if the underlying data is incomplete, delayed, or inconsistent, which is why data quality in healthcare is a direct lever for better detection.
High-quality chronic disease identification is a system decision with operational consequences. It defines who is on a chronic trajectory, where the patient is on that trajectory, and which protocol is appropriate for the current stage. The business risk is measurable: Medicare’s Hospital Readmissions Reduction Program allows for payment reductions up to 3%, making preventable readmissions a direct threat to reimbursement stability.
A reliable identification layer also prevents “single-signal” classification. Many chronic conditions require repeated or multi-criteria confirmation before you can treat them consistently. Hypertension is a practical example: diagnosis is based on repeated measurements across multiple visits, and guidelines also support out-of-office measurements when feasible.
Kodjin Analytics supports this multi-factor, longitudinal approach by helping teams build explainable chronic cohorts from time-linked clinical and utilization signals, then operationalize them as worklists and stage-based pathways that clinical leaders can trust and act on.
How Hospitals Protect Reimbursement and Stabilize Utilization with the Help of Advanced Healthcare Analytics
Hospitals view chronic disease as utilization volatility and direct financial exposure. In 2018, the U.S. had 3.8 million adult 30-day readmissions, with an average cost of $15,200 per readmission, and Medicare accounted for 2.3 million of those readmissions.
Readmission prevention becomes targeted
High-quality detection helps hospitals focus transition work on the chronic cohorts most likely to rebound, rather than running generic discharge actions for everyone. Kodjin Analytics supports that by enabling stable cohort definitions, time-based risk visibility, and cohort behavior tracking over time.

Capacity planning becomes more predictable
Chronic patients create recurring demand with patterns. When cohorts are stable and stage-aware, leaders can forecast bed days, follow-up volumes, and care management load with less variance. Kodjin Analytics supports longitudinal trend views, so planning is based on timelines rather than snapshots.
Pathways become easier to control
Once cohorts are consistent, hospitals can compare what happens next across similar chronic subgroups and stage bands, then adjust pathways to reduce complications, long stays, and returns. Kodjin Analytics supports this kind of cohort and pathway analysis without turning every question into a custom data project.
How Clinics Turn Early Recognition into Consistent Protocol Decisions
In ambulatory care, clinicians often suspect chronic disease earlier, but choosing protocols becomes harder as complexity increases. Given the prevalence of multimorbidity, consistency requires multi-criteria detection that can be tested across populations.This is where population health analytics becomes practical: stable cohorts, stage-aware segmentation, and measurable interventions over time.
Complex cases need longitudinal context
Symptoms overlap, comorbidities shift risk, and therapy can improve one signal while progression continues elsewhere. Kodjin Analytics supports multi-criteria cohorts that reflect real patient history, so protocol decisions are anchored in longitudinal context rather than single indicators.
Medication response and adherence belong in the identification quality
Chronic control often fails quietly. CDC reports that one in five new prescriptions is never filled, and about 50% of filled prescriptions are taken incorrectly. Nonadherence is associated with $100–$300B in avoidable costs annually.When medication timelines are connected to outcomes and utilization, clinics can spot “treated but unstable” subgroups and refine protocols based on real-world response.
Faster iteration reduces protocol drift
Protocol quality improves when clinical leaders can test cohort logic and validate subgroup behavior without long waits. Kodjin Analytics is built for self-serve exploration and reusable cohort logic, which helps clinics standardize decisions across providers.
How Integrated Delivery Systems Reduce Losses During Care Transitions
Integrated delivery systems have a unique advantage because they can manage chronic trajectories across settings. The largest operational losses often happen during transitions, when follow-up is delayed, medication changes are misunderstood, or risk signals are missed after discharge.
The core requirement is shared identification logic. If the clinic and the hospital define “chronic” differently or stage patients differently, the system cannot run consistent transition workflows or measure outcomes reliably across the continuum. This is also why healthcare data standards matter: they help maintain consistent meaning across sources and reduce drift in definitions as data moves between systems.
Kodjin Analytics helps by keeping cohort definitions consistent across settings and supporting longitudinal visibility that follows the patient across the care continuum. That enables care transitions and readmission-prevention workflows driven by the same chronic definitions used for hospital risk staging and clinic protocol planning.
High-Quality Chronic Disease Detection: What It Takes to Get It Right
At a leadership level, identification becomes “high-quality” when it delivers three things consistently.
1) Analytics access that clinical teams can use without bottlenecks
Chronic disease detection cannot depend on long request cycles and one-off queries. Clinical leaders, care management teams, and operational managers need the ability to explore cohorts, validate logic, and refine definitions quickly, because chronic trajectories change over time and programs evolve. Kodjin Analytics supports this self-serve workflow through explainable cohort building and interactive exploration, so teams can work with data directly and move faster from question to action.
2) Longitudinal context that stays intact
Chronic disease is time-based by definition. The Centers for Disease Control and Prevention (CDC), a public health agency within the Department of Health and Human Services (HHS), describes chronic diseases as conditions that last one year or more and require ongoing medical attention or limit the activities of daily living. Your identification logic needs to account for patient history, trends, and timing. Kodjin Analytics supports longitudinal analytics, enabling teams to work with timelines rather than isolated events.
3) Multi-criteria logic that reflects real-world complexity
Single-signal thresholds are fragile. Real cohorts usually need repeated signals, persistence over time, comorbidity context, and therapy response. Complexity is common at scale: a CDC analysis reported that 42% of U.S. adults have two or more chronic diseases. Kodjin Analytics supports cohort logic and pathway analysis on time-linked data, which fits multi-factor detection for chronic conditions management.
4) Staging that turns identification into operations
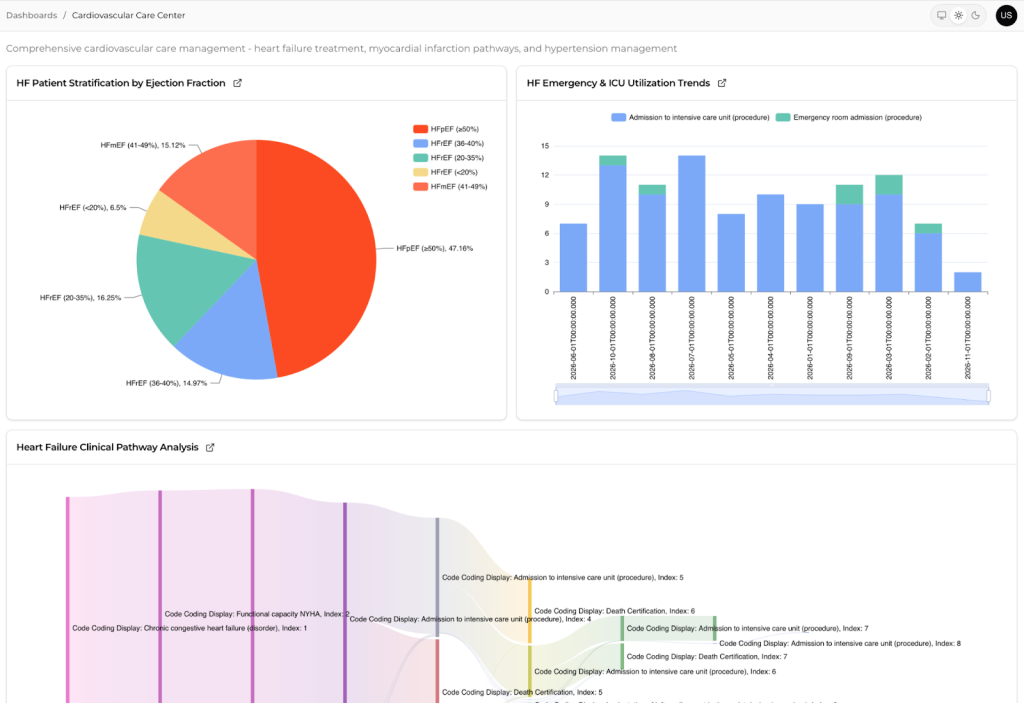
“Chronic” is not one state. Stage changes monitoring intensity, escalation thresholds, care management cadence, and expected utilization. Kodjin Analytics helps teams translate cohorts into stage distribution views and patient-level timelines that support action.
How Kodjin Analytics maps this into day-to-day execution
Kodjin Analytics supports a practical identification-to-action workflow that does not depend on ad hoc reporting. The product’s value shows up when cohort definitions are explainable, reusable, and tied to operational views that teams can execute consistently.
| Step into a high-quality workflow | What the team is trying to do | How Kodjin Analytics supports it |
| Define the chronic cohort | Convert “possible chronic” into an explainable definition | Cohort building designed for time-linked insight and clinical context |
| Validate longitudinal patterns | Confirm persistence, progression signals, and comorbidity context | Longitudinal outcomes and time-aware analysis across patient history |
| Stage the population | Separate early-stage from advanced-stage pathways | Cohort segmentation that supports stage-based monitoring and planning |
| Operationalize the cohort | Turn cohorts into worklists and pathway monitoring | Reusable cohort logic that can be applied consistently across teams |
| Measure impact | Track utilization, outcomes, and cost movement by cohort and stage | Views that connect care, cost, outcomes, and population trends |
When organizations rely on multiple systems, consistent cohort logic depends on normalized data. The Kodjin FHIR® Server can act as an interoperability layer that helps unify input data for analytics.

Conclusion
High-quality chronic disease detection is a foundation for predictable operations and better financial performance. When detection is longitudinal, multi-criteria, and stage-aware, organizations can target interventions earlier, manage transitions more consistently, and measure impact with cohorts that stay stable over time.
Kodjin Analytics supports this approach by making complex chronic detection practical at scale through explainable cohorts, longitudinal pattern detection, and reusable logic that teams can operationalize across hospitals, clinics, and integrated systems.
FAQs
How do we know our chronic disease management metrics are driving real outcomes?
Metrics drive outcomes when they support chronic disease case management decisions that people can execute. Tie each metric to a specific action, a clear owner, and a follow-up cadence. Use stable cohorts, track who received which intervention, and measure changes in utilization, complications, and total cost of care versus a baseline period or a comparable cohort.
When does investing in a healthcare data platform become necessary for chronic disease management?
A platform becomes necessary when chronic care relies on data spread across multiple systems, and teams cannot get a consistent patient story fast enough. Common triggers include repeated readmissions, inconsistent cohort definitions across departments, limited ability to stage patients, and heavy dependence on analysts for routine changes. At that point, scaling chronic health management requires a shared data foundation and governed definitions.
What level of interoperability is required to track chronic disease outcomes accurately?
You need enough interoperability to follow the patient across settings and time with consistent meaning. At minimum, that includes EHR clinical data, labs, medications, encounters, and claims or utilization signals, linked to a reliable patient identity. Standardized models and governance matter because they keep measures consistent across sources and support comprehensive disease management across the continuum.
How long does it typically take to operationalize chronic disease metrics with an integrated data platform?
Timelines depend on data readiness and scope. Many organizations can deliver initial cohorts and core dashboards in a few weeks once key feeds are connected and validated. A mature setup usually takes a few months, especially with multiple sites, because the chronic care management model needs stable cohort definitions, refresh automation, and workflow alignment.
How can chronic disease management metrics justify long-term investment in data and analytics platforms?
The strongest business case ties metrics to financial levers leadership already tracks: avoidable utilization, readmissions, capacity volatility, and total cost-of-care trends for defined cohorts. Long-term value becomes clear when earlier detection and stage-based interventions reduce expensive episodes over time, stabilize planning, and improve performance in value-based contracts, with results measured consistently quarter over quarter.
How does Kodjin support long-term chronic disease programs beyond initial data integration?
Kodjin supports long-term programs by keeping cohort logic stable, explainable, and reusable as definitions evolve. Teams can refine multi-criteria cohorts, apply staging, compare subgroup pathways, and monitor trends over time without rework. That helps programs stay operational as populations shift, guidelines change, and new data sources are added, while maintaining consistent measurement across clinics, hospitals, and care management teams.