If you run a multi-site health system, you already know: the patients who need care most are often the hardest to keep track of, and the most expensive when you lose sight of them. For medium-to-large providers, keeping care strong and budgets stable go hand in hand. And the people who test the system most are often the ones who need it most — vulnerable patient populations, where biology, social factors, and financial barriers overlap.
Think of infants, older adults, people with chronic disease or disability, ethnic minorities, LGBTQ+ communities, survivors of violence, veterans, people without homes, and anyone who can’t access care consistently―these are some examples of vulnerable populations in healthcare. The right approach is not to avoid “expensive” patients but to build a strategy for early identification and support that protects people while improving financial performance.
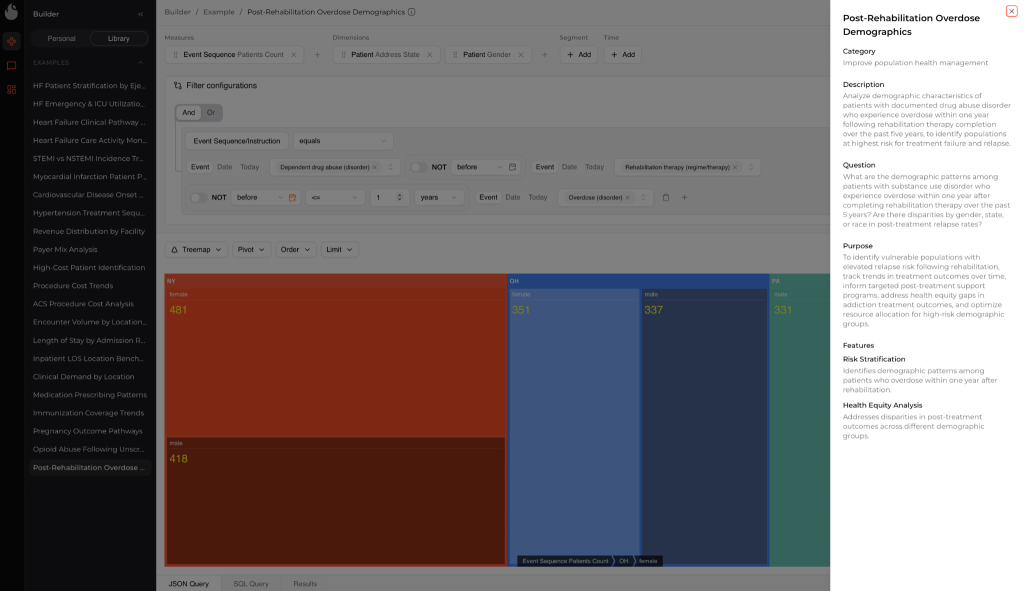
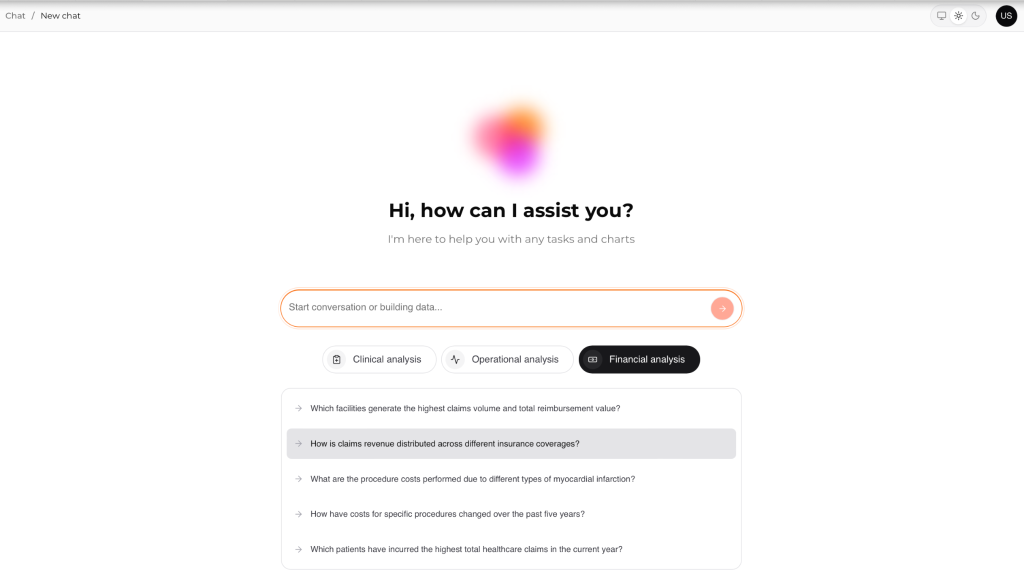
Below, we explore how to define a vulnerable population in healthcare, why it matters, and how Kodjin, custom medical analytics software, turns data into action. To identify sensitive groups, you simply ask a natural‑language question to uncover the necessary patterns, rather than relying on a single parameter.
Highlights:
- Each year in the U.S., there are over 3.8 million hospital readmissions. On average, each readmission costs about $15,200.
- Medication nonadherence costs the U.S. $100–$300B each year and is linked to avoidable hospitalizations and deaths.
- Insurance coverage, transportation, housing, education, and social support influence access to healthcare and treatment outcomes.
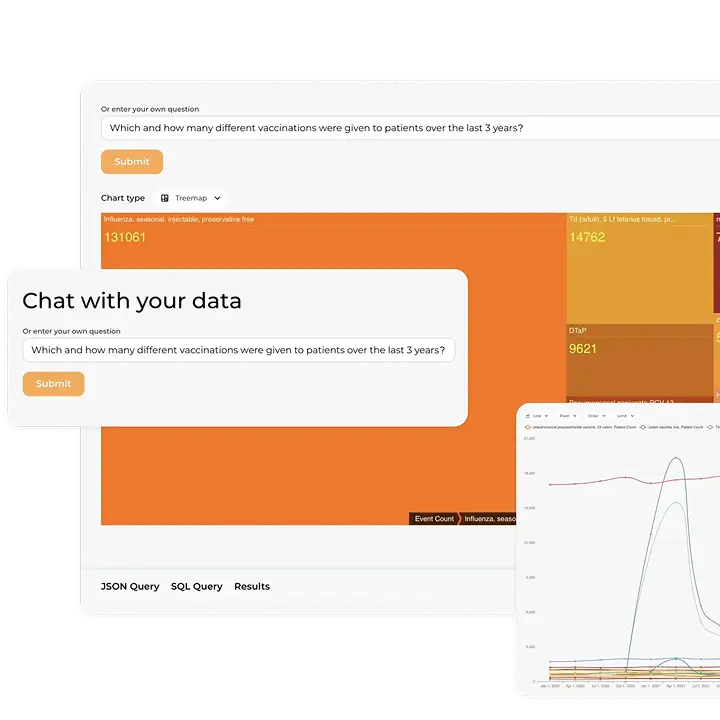
Explore our Conversational Healthcare Software
Learn more
What Makes a Patient Vulnerable?
Healthcare vulnerability rises when medical risk meets barriers in daily life. That overlap increases the chance of harm, complications, or avoidable hospital visits. It is rarely a single warning sign. More often, it’s a pattern across health status, social context, and habits. That’s why two people with the same diagnosis can have very different outcomes. In practice, providers work with different types of patient populations, and vulnerability looks different in each.
Clinical vulnerabilities
Clinical vulnerability means medical complexity and low physiologic reserve. The risk climbs when conditions stack up, symptoms flare often, or the patient’s baseline is fragile.
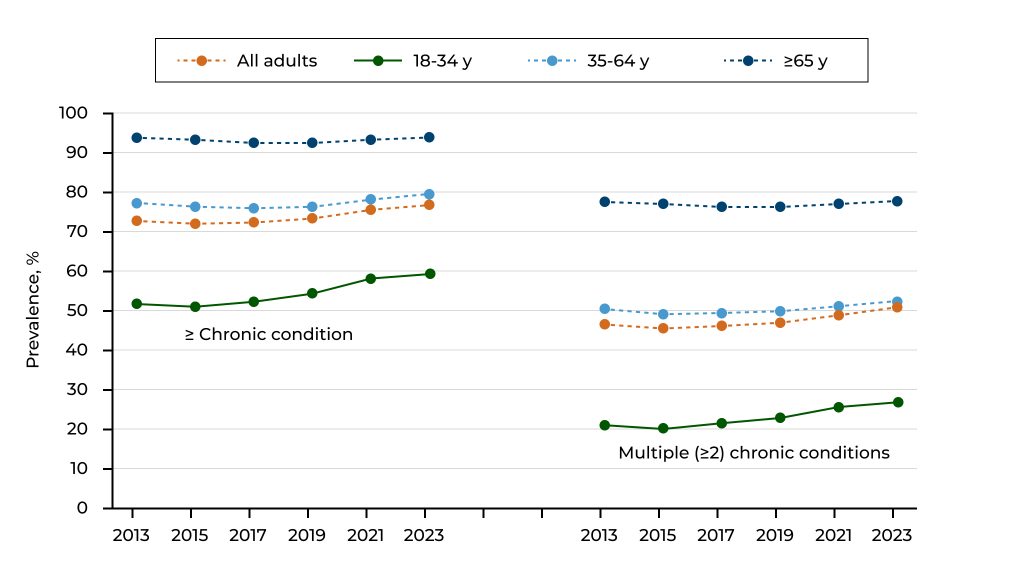
- Multiple chronic conditions (MCC) affect many people. In 2023, 51.4% of individuals in the U.S. reported having more than one long-term health problem. The rate was even higher for older adults at 78.8%.
- If a person is weak, elderly, or taking many medications, the problem can worsen very rapidly, even if it’s small. For instance, a simple infection could produce delirium, a new prescription could make someone collapse, and not going to a follow-up visit could evolve into an emergency.
Clinical vulnerability also looks different across settings. In an emergency department (ED), it may manifest as repeat visits, short-interval returns, or worsening vitals across encounters, even if each visit appears “manageable”.
Kodjin unifies clinical data across episodes of care, so teams can see longitudinal histories of diagnoses, medications, lab results, and encounters. The semantic layer allows you to define cohorts, such as “older adults with three or more chronic conditions,” once and reuse them across dashboards. By tracking medication changes and emergency department (ED) encounters over time, Kodjin highlights patterns that point to frailty or polypharmacy risks.
Example prompts to try with Kodjin’s AI Assistant:
- Which patients over the age of 65 have visited the emergency department three or more times in the past year and are currently taking at least five medications?
- Locate patients who have chronic kidney disease and diabetes and whose blood pressure has increased in the past three encounters.
- List patients who were discharged following an acute incident and failed to attend their specialist follow-up appointment within 14 days.
Social & environmental vulnerabilities
Social and environmental vulnerability refers to a patient’s ability to access care and follow a plan. These factors represent barriers to healthcare in a vulnerable population.
- Medical care is estimated to contribute only 10-20% of the modifiable drivers of health outcomes, while the remaining 80-90% is tied to social, behavioral, and environmental factors (often grouped as social determinants of health (SDOH)).
- 5% of all U.S. adults reported forgoing healthcare due to transportation barriers, and 21% of adults without access to a vehicle or public transit went without needed medical care
Some common indicators include unstable housing, insufficient food, language difficulties, absence of social support, gaps in insurance coverage, and difficulty accessing primary care. These problems can make it difficult to get care, make it harder to stick to therapy, and disrupt regular care.
Kodjin adds SDOH indicators to clinical records, such as ZIP code-level poverty, insurance status, and social risk assessments. You can filter and view patients by these factors and clinical data to spot those who may have trouble making appointments or following care plans. The platform also supports natural language queries, so anyone can combine social and clinical criteria without writing code.
Example prompts to use:
- Identify patients with uncontrolled hypertension who live in areas where public transportation is limited and have missed at least two appointments in the last six months.
- List all pregnant patients who do not have insurance and reported food insecurity during their intake.
- Which patients in the heart failure registry also have housing instability noted in their records?
Behavioral & lifestyle vulnerabilities
Behavioral vulnerability refers to patterns that affect how a person handles their daily care. The goal is to suggest a care plan that could offer extra support, simpler steps, or a different way to check in.
Medication adherence is one of the biggest drivers. One research study estimates medication nonadherence costs $100-$300 billion per year in the United States and associates it with substantial avoidable hospitalizations and deaths.
Mental health issues, substance use, cognitive problems, and low health literacy can all make it harder for patients to follow through, even if they want to. These challenges often show up as missed refills, irregular monitoring, skipped appointments, or repeated emergency department visits after discharge.
Kodjin aligns the pharmacy and behavioral signals with clinical history. It shows missed pick-ups and refill gaps, tracks screening scores, and places those trends alongside readmissions and ER visits. So care teams can spot “this patient is slipping” earlier and bring in pharmacy or behavioral health support before it turns into another acute visit.
Example prompts to use:
- Which patients with depression scores over 10 on the PHQ‑9 have missed two or more antidepressant refills in the last quarter?
- Identify patients with chronic obstructive pulmonary disease who have not refilled their inhaler prescriptions on time and have had an unplanned admission in the past six months.
- Show me patients with two or more ED visits for substance‑use‑related issues who have not been contacted by a behavioral health specialist.
Kodjin can link prescription data, refill histories, and behavioral‑health diagnoses to clinical events. It flags gaps in medication pick‑ups, tracks PHQ‑9 or other screening scores, and correlates them with readmissions or emergency visits. This enables care teams to quickly identify the most vulnerable populations who may need extra support or outreach from behavioral health and pharmacy teams.
Why Identifying Vulnerable Patients Matters
When vulnerability stays invisible, it later manifests as avoidable crises, repeat visits, and team burnout. Early identification helps you act while there is still time to change the trajectory, especially in systems that run a clinic, a hospital, and an emergency department. This is the same logic that powers data analytics in population health management: you’re tracking risk signals over time and across settings.
Improve patient outcomes and safety
Vulnerable patient identification helps prevent harm by identifying risk patterns before they become complications.
Our product brings clinical and non-clinical signals together in one place and lets staff explore them without technical support. It uses a semantic layer and a natural-language assistant, so teams can ask business-level questions and see time-linked risk signals across the patient journey.
Reduce hospital readmissions and costs
Hospital readmissions are expensive and often predictable if you can see the pattern early. In the United States, an estimated 3.8 million readmissions occurred in 2018, with an average cost of $15,200 per readmission.
Time-linked insights across multiple use cases support risk stratification and early outreach. This matters when risk is not a single event but a sequence of events, such as repeated emergency department visits, missed follow-ups, and unstable vitals over time. Kodjin Analytics is built to surface these longitudinal patterns without forcing teams to rebuild logic for each use case.
Ensure regulatory compliance and ethical care standards
Readmissions are not only a clinical issue. They are also a reimbursement and reporting issue. Under the Centers for Medicare & Medicaid Services (CMS) Hospital Readmissions Reduction Program (HRRP), the payment reduction is capped at 3%.
Our product supports consistent cohort definitions and repeatable logic through its semantic layer and conversational access. That makes performance tracking and internal reporting easier to defend across teams and sites.
Enable proactive, personalized care
A small share of patients typically accounts for a large share of costs and utilization. In 2022, people in the top 5% of the expenditure distribution accounted for about 49.7% of healthcare expenses in the United States.
Teams can identify high-risk cohorts fast and translate them into clear next steps for outreach and care coordination with Kodjin Analytics. It also reduces reliance on analyst queues because staff can explore the data in plain language.
How Kodjin Helps Identify Vulnerable Patients
Vulnerability is rarely noticeable immediately. It develops over time through different encounters, lab results, medications, how care is used, and a person’s social situation. Kodjin Analytics helps you bring those signals together, so teams can spot risk earlier and act with confidence.
Democratized insights for every user
Kodjin is designed to democratize access to analytics. Care coordinators, nurses, and other non-technical staff can use the platform’s language assistant to ask questions. The platform provides clear lists and trend lines, eliminating the need for SQL or data team support.
Cohorts and measures are versioned and reusable. Once you agree on what “high-risk discharge” means, it stays consistent everywhere. The same definition shows up in dashboards, patient lists, and reports, so teams don’t argue over labels. Kodjin brings those insights into the EHR and care tools you already use. Alerts and worklists land where staff actually work, without another portal to check. Signals come through near real time, when timing matters most. For example, right after discharge or ahead of a follow-up visit.
Integrated data analytics
Kodjin brings together clinical, operational, and social data into a single platform. The system consolidates electronic health records, registries, billing data, and other sources into a unified, continuous record, regardless of whether the data uses FHIR®, HL7 v2, CDA, or flat-file formats. This enables providers in clinics, hospitals, and emergency departments to access comprehensive information without relying on a single standard. Optimal performance is achieved when data is hosted on a FHIR® server, enabling groups, measures, and alerts to follow a consistent structure rather than rely on custom configurations.
It also supports multiple integration paths (for example, Health Level Seven (HL7) version 2, Clinical Document Architecture (CDA), flat files, and Fast Healthcare Interoperability Resources (FHIR®)), which matters for providers that still run mixed environments across clinic, hospital, and emergency department workflows.
If your data is spread across systems, you’re not alone. Explore the common challenges of data analytics in healthcare and how teams address them.
Turning Insights into Action with Kodjin
Identifying vulnerable patients is step one. The real value comes when the insight becomes a repeatable workflow: a clear outreach list, an owner, and a follow-up loop.
Personalized care plans for high-risk patients
With Kodjin, teams can turn risk patterns into patient-specific next steps. For example, identifying a “high-risk discharge” cohort can initiate a standard bundle that includes a 48-hour follow-up call, medication reconciliation, enrollment in remote monitoring, and a scheduled follow-up appointment.
Reusable cohorts and measures ensure consistency across departments and facilities, preventing variations in the definition of “high risk” among teams.
Coordinated care across multidisciplinary teams
Because vulnerability impacts multiple areas, interventions should be comprehensive. Kodjin’s shared worklists help care coordinators, nurses, social workers, and service-line leads align outreach efforts and address common barriers such as transportation, follow-up access, and coverage gaps.
This is especially relevant for providers with clinic, hospital, and emergency department care under one roof, where handoffs and follow-ups are where patients often fall through the cracks.
Risk scoring & prioritization
Once data is unified, Kodjin helps you move from “who is eligible” to “who is at risk next.” You can define cohorts and measures once and reuse them across dashboards, operational lists, quality programs, and analytics work.
For risk scoring, the point is not just a number. Teams need to understand why a patient was flagged. Kodjin supports transparent logic, including visibility into cohorts, features, and thresholds, and it can support clinician override when needed.
Scores aren’t enough if staff can’t act quickly. See what good healthcare data visualization looks like for risk timelines, care gaps, and prioritization.
Tracking outcomes to continuously refine prioritization
Kodjin helps teams connect actions to outcomes over time, then refine thresholds and cohorts based on what actually changes utilization and safety. It supports versioned measures and governance so the organization can evolve its logic without losing compatibility.
For example, in the Zoadigm case, a FHIR®-native semantic-layer analytics platform helped specialty practices unify messy clinical data and make cohort discovery practical for non-technical users. The published results showed that the platform supported a 9× higher volume of matched patients for clinical trials than for regular screening.

What matters for your vulnerable patient workflow is the mechanism: the same “longitudinal patient view + reusable cohort logic + self-service exploration” approach can help staff spot multifactor risk patterns earlier, then turn them into prioritized worklists and consistent follow-up actions.
Best Practices for Managing Vulnerable Patients
Identifying vulnerable patients is the start. What matters is what you do next. Define risk criteria, monitor continuously, and follow up fast. Close the loop by tracking results and adjusting. That’s how teams intervene sooner and coordinate care better.
Standardize risk assessment protocols
If teams use different definitions of “high risk,” you get uneven care and conflicting reports. Use one vulnerability model across the org. Mix clinical signals, SDOH, and behavioral factors into a single playbook. Then, agree on a short list of cohorts everyone will use, like repeat ED visits, no follow-up after discharge, uncontrolled chronic markers, or high social risk. Version those definitions, so it’s always clear what changed and why.
Start with one shared vulnerability model that covers clinical signals, social determinants of health (SDOH), and behavioral factors. Then choose a small set of standard cohorts you will rely on across the organization, such as frequent emergency department visits, post-discharge patients without follow-up, uncontrolled chronic condition markers, or high social risk. Keep those definitions versioned, so everyone knows what changed and why.
Kodjin Analytics standardizes healthcare data from multiple formats, FHIR®, HL7 v2, CDA, flat files, and more, and applies a governed semantic layer, enabling cohorts and measures to be defined once and reused across dashboards, operational lists, and care programs.
Before you scale vulnerability programs, make sure your inputs are reliable. See why the importance of data quality in healthcare is the foundation for accurate risk identification.
Monitor patients proactively with near-real-time signals
Vulnerability usually shows up as a trend. The goal is to catch it before it becomes an avoidable return visit. Focus on time-based patterns, like repeat visits, missed labs, escalating medication changes, or unresolved abnormal vitals, rather than single data points. Pay special attention to transition moments where patients often fall through the cracks, including emergency department discharge, inpatient discharge, referrals, and care handoffs. Build a consistent review cadence for high-risk lists, based on how fast your patient population changes.
Kodjin Analytics supports time-linked analysis of standardized data, enabling teams to query longitudinal journeys and spot risk sequences early.
Engage patients and caregivers with targeted interventions
A standard education workflow is rarely enough for vulnerable patients. Interventions need to match real barriers. Segment outreach by the reason support is needed: transport, language, medication confusion, caregiver gaps, or mental health needs. Use simple, repeatable intervention bundles so staff can act fast and consistently, and involve caregivers early when adherence, cognition, or mental health is part of the picture.
Kodjin Analytics can generate prioritized worklists based on combined clinical and SDOH signals, so teams focus outreach on the patients most likely to benefit now.
Continuously evaluate outcomes to improve care plans
Without feedback loops, care management becomes an activity without clarity. Tie each program to a few measurable outcomes, review false positives and missed cases regularly, and refine thresholds based on what actually changes results. Keep governance clear: who approves cohort changes, how often updates happen, and how impact gets documented.
Kodjin’s semantic layer supports consistent, traceable cohort logic, which makes it easier to compare outcomes over time and refine prioritization without rebuilding metrics from scratch.
Conclusion
The business model of successful healthcare providers depends not only on financial stability but also on fulfilling a social mission. Vulnerable patients need extra attention and support. A strategy of early identification, comprehensive data use, and predictive analytics enables providers to improve the quality of care, reduce costs, and enhance patient loyalty.
Kodjin Analytics equips organizations with tools to transform disparate data into structured knowledge and provides an AI assistant that helps staff draw strategic conclusions. Studies show that using machine learning and multifactor models lowers the risk of readmissions and enables individualized care plans. Thus, investing in vulnerable patients is a step toward a fairer, higher‑quality, and more financially sustainable healthcare system.
FAQs
How does Kodjin integrate into existing healthcare workflows?
Kodjin is designed to fit alongside your current systems rather than replace them. It ingests data from EHRs, registries, billing feeds, and ancillary systems, harmonizing them regardless of whether they use FHIR®, HL7 v2 messages, CDA, or flat‑file formats. These disparate feeds are transformed into a longitudinal record with consistent semantics. Through its semantic layer, cohorts and measures defined once automatically appear in dashboards, operational lists, and quality reports. Kodjin doesn’t force users into another portal: alerts and worklists surface inside the EHR and care‑management tools staff already use, and non‑technical users can pose plain‑language questions.
How does Kodjin support population health initiatives?
Population health work depends on consistent cohorts and repeatable rules. Kodjin helps you define populations once (for example, “high-risk discharges” or “frequent emergency department users”) and reuse that logic across programs, reporting, and follow-up workflows. It’s also useful when you need to spot patterns over time, especially for vulnerable patients whose risk builds across visits, labs, meds, and missed follow-ups.
How secure is patient data in Kodjin?
Our security is built around practical controls: encryption, strong authentication, granular access policies, and audit trails, so you can see who accessed what and when. It’s designed to support compliance with the requirements of healthcare environments, including the Health Insurance Portability and Accountability Act (HIPAA) and the General Data Protection Regulation (GDPR), depending on your region and setup.
Is your platform suitable for insurance providers and payers?
Yes, payers often need to combine clinical signals with administrative and financial data to run care management, risk adjustment, utilization analytics, or value-based care reporting. Kodjin can work with payer-side formats like Accredited Standards Committee X12 (ASC X12), alongside clinical standards such as FHIR®, so you can analyze member journeys across settings rather than relying solely on claims.
How can AI help identify vulnerable patients sooner?
Many care teams still rely on fixed risk scores, manual chart reviews, or reports that only show patients once they already match a known high-risk profile. AI can help teams see risk earlier by connecting clinical history, service use, social factors, and behavioral patterns in one place. This makes it easier to notice when a patient’s situation starts to change, even before they reach a formal risk threshold. With Kodjin, care managers can work with unified patient data through a semantic layer and ask practical questions in plain language. For example, they could search for diabetic patients with transportation barriers who have not seen a primary care provider in six months. Instead of waiting for a static report, they can get answers quickly and use that time to close care gaps before a preventable hospitalization happens.
What is the best clinical strategy for early detection of vulnerable patients?
The strongest strategy is usually a mix of good data, regular monitoring, and clear clinical action. Healthcare organizations need to look beyond diagnosis codes and combine EHR data, claims, SDOH screenings, utilization patterns, and behavioral signals to understand which patients may need support sooner. Early detection also works better when it happens continuously, not only during scheduled reviews or quarterly reporting cycles. The data should reach care teams in a form they can use right away, without depending on analysts for every cohort update or risk-factor change. Kodjin helps with this by letting teams build and adjust vulnerable population cohorts, test new criteria as needs change, and move findings into care management workflows where they can guide outreach, follow-up, and intervention.