Medical knowledge forms the core of EHRs, and to represent this knowledge, patient data needs to be captured from multiple sources, including problem lists, procedures, medication lists, laboratory results, and more. However, the use of natural language in EHRs can create ambiguity and a lack of standardization. To address this, healthcare stakeholders have developed standardized FHIR terminology modules and classifications that help in the codification and standardization of medical concepts.
In recent years, the healthcare industry has seen the emergence of the Fast Healthcare Interoperability Resources (FHIR) standard, which includes a terminology module to support the use of standardized terminologies. The use of the FHIR terminology module helps enhance the accuracy and consistency of data exchanged between healthcare providers, payers, and other stakeholders, ultimately leading to better patient outcomes.
In this article, we will have a terminology introduction process and explore how healthcare terminologies facilitate the standardization of clinical data and its exchange, provide examples of various terminologies, and examine the FHIR Terminology Module and how it works.
What Are Healthcare Terminologies?
Terminology in healthcare refers to a set of standardized terms and codes used to represent medical knowledge and patient data in electronic health records (EHRs). The goal of using terminology in EHRs is to increase patient safety, reduce medical errors, improve efficiency, and more. Terminology helps to resolve ambiguities and standardize vocabulary, which is necessary for capturing clinical data in a structured and preferably coded format.
Codification in this case is the process of reducing a concept into a code, usually numeric or alphanumeric. Standard codification systems, such as classifications (ICD-10, CPC, LOINC, etc.) or terminologies (SNOMED-CT), are used to represent facts that happen in the real world in a way that can be managed in a database.
Terminologies are made of formal aggregations of language-independent concepts represented by one favored term and appropriate synonymous terms and of explicitly represented relationships among the concepts. The use of standard terminologies in an EHR is useful to enable decision support systems, exchange data between health information systems, perform epidemiological analysis, support health services research, and manage administrative tasks, among others.
At the same time, organizations must consider the challenges of healthcare data privacy to safeguard sensitive patient information while using standardized terminologies across multiple systems.
While many terminologies have been developed, no single terminology has been accepted as a universal standard for the representation of clinical concepts.
Terminologies used in healthcare
Proper understanding and utilization of terminologies are essential for facilitating effective communication, improving patient care, and enabling the use of electronic health records (EHRs) to their fullest potential. There are several healthcare terminologies available, each with its own unique features and intended uses. Below, we will describe some of the most commonly used healthcare terminologies, including SNOMED CT, LOINC, and ICD-10, among others.
- SNOMED CT: Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) is a comprehensive, multilingual clinical terminology used to describe medical concepts and provide a standardized language for healthcare communication. SNOMED International, a non-profit organization responsible for developing and distributing SNOMED CT, operates under the International Health Standards Development Organization.
SNOMED CT consists of a set of coded terms that can be used within EHRs to capture, record, and exchange clinical data, facilitating the retrieval of useful clinical information. It is an essential component of FHIR-based solutions that support the use of clinical data in healthcare organizations.
- LOINC: Logical Observation Identifiers Names and Codes (LOINC) is designed to facilitate the sharing and pooling of results, such as laboratory tests or vital signs, for use in clinical care, outcomes management, and research.
LOINC is widely regarded as a universal coding system, allowing healthcare organizations to connect their local codes to LOINC codes for transmission in clinical messages to payers, regulators, and other healthcare organizations. LOINC codes are unique, six-part identifiers that not only identify the component being measured (such as Hemoglobin) but also the specimen type (such as whole blood) and other defining characteristics of the result.
- ICD-10: The International Statistical Classification of Diseases and Related Health Problems (ICD) is a medical classification system developed by the World Health Organization (WHO). ICD-10, its 10th revision, contains a vast range of codes that provide vital information on a variety of health-related topics.
These codes cover abnormal findings, complaints, diseases, epidemiology, external causes of injury, managing health, treating conditions, signs and symptoms, and social circumstances. In total, there are over 14,400 codes in ICD-10, which can be further expanded to more than 16,000 codes when optional sub-classifications are used.
- RxNorm: RxNorm is a standardized nomenclature for clinical drugs and drug delivery devices. It provides a way to standardize medication names across different healthcare systems and allows healthcare providers to easily identify and track medications.
Various hospitals, pharmacies, and organizations use different names to refer to identical medications, including both generics and branded drugs. To reduce confusion and promote consistency, the National Library of Medicine (NLM) developed and currently maintains RxNORM. Its goal is to provide a uniform format for the names of drugs.
Read Also: Data Interoperability in Pharmaceutical
What Is a FHIR Terminology Module?
FHIR is a standard framework created by HL7 to provide easier and quicker implementation of interoperability in healthcare systems to facilitate access to healthcare data stored in multiple EHRs/HIT systems.
The FHIR specification introduces the FHIR Terminology Module, which “lets healthcare applications make use of codes and value sets without having to become experts in the fine details of code system, value set, and concept map resources, and the underlying code systems and terminological principles.”
As such, it provides a way to define, manage, and distribute terminology artifacts (code systems, value sets, and maps), which are essential for accurate and consistent representation of clinical concepts. Let’s closely examine how these artifacts are implemented in FHIR.
To fully grasp how these terminology artifacts interact within healthcare applications, it’s helpful to review understanding FHIR components, which explains the structure and relationships of FHIR resources in practical scenarios.
Components of the FHIR Terminology Module
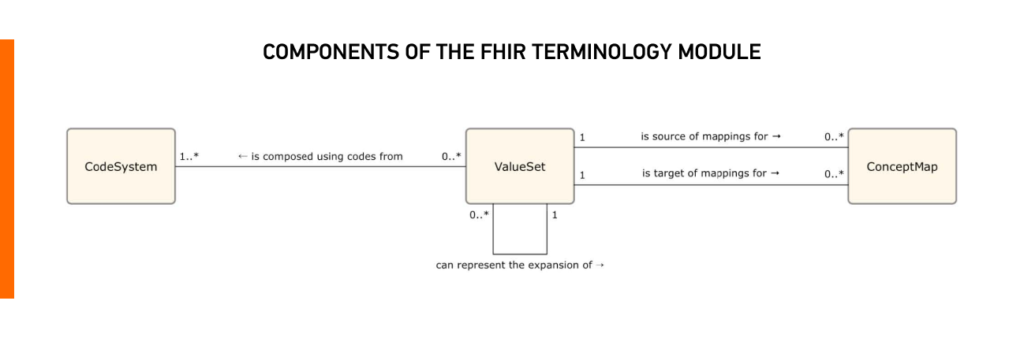
The FHIR Terminology Module has three main components: code systems, value sets, and concept maps. Each of these components also has defined operations that can be performed with them, which we will describe in more detail below.
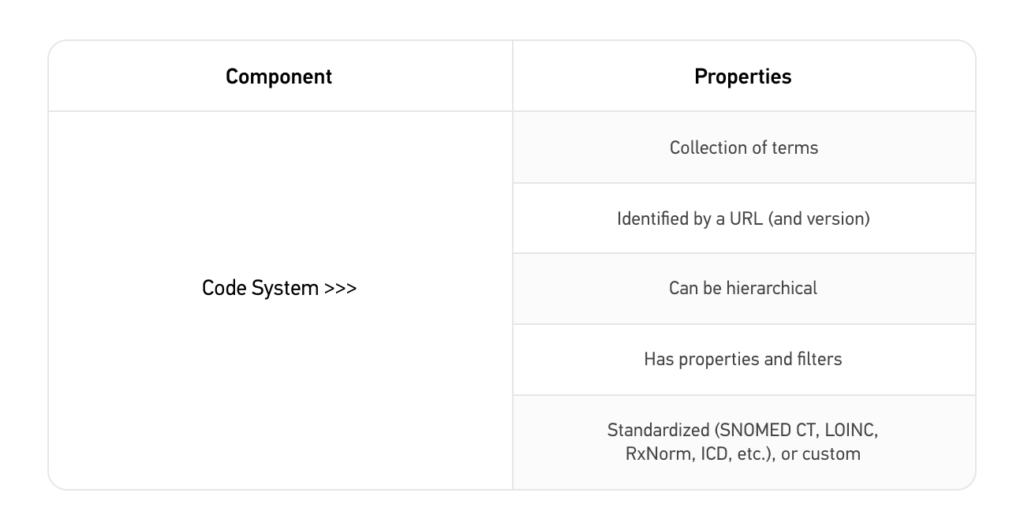
Code system
A code system is a set of codes that represents a specific medical concept, such as a disease or procedure. Each code has a unique meaning and is used to identify a particular concept. Examples of code systems include SNOMED CT, LOINC, and ICD-10.
CodeSystem Operations
$lookup
The $lookup operation provides a way to retrieve specific information (code/system/version or coding) about a code within a code system. It can also be used to check if a specific code exists within the CodeSystem.
$subsumes
The $subsumes operation provides a way to determine whether one code is subsumed by another code, i.e., whether the meaning of the first code is fully included in the meaning of the second code.
The $subsumes operation can be used in a variety of clinical and administrative scenarios, such as decision support, coding and billing, and quality reporting. For example, a healthcare provider may use $subsumes to determine if a more specific code for a condition is subsumed by a broader code required for billing or reporting purposes.
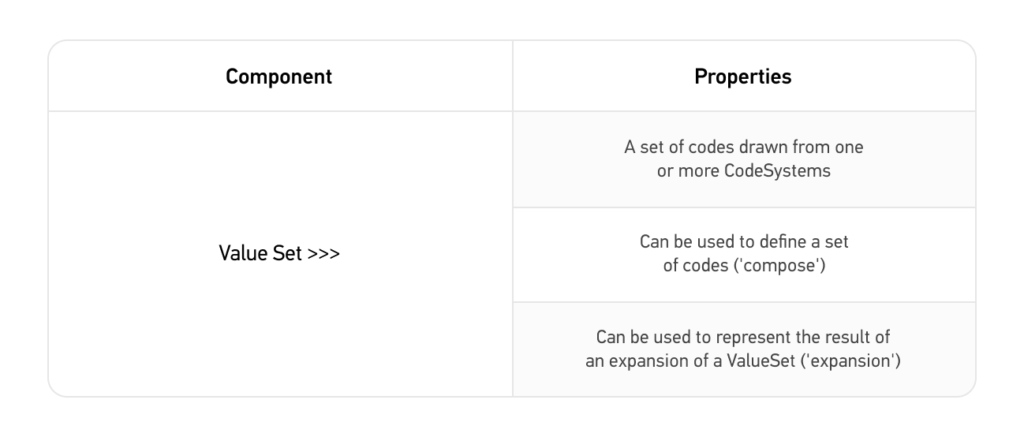
Value set
A value set defines a group of concepts applicable in certain contexts. It can draw codes from one or more CodeSystem.
ValueSet operations
$expand
The operation $expand can retrieve a set of codes defined by a ValueSet and any hierarchical relationships between those codes. This is typically the main way to search for a code.
$validate-code
The $validate-code operation provides a way to validate whether a code is valid according to a specified ValueSet or is used to check if a code is included in the ValueSet. This is the main method for validating coded data.
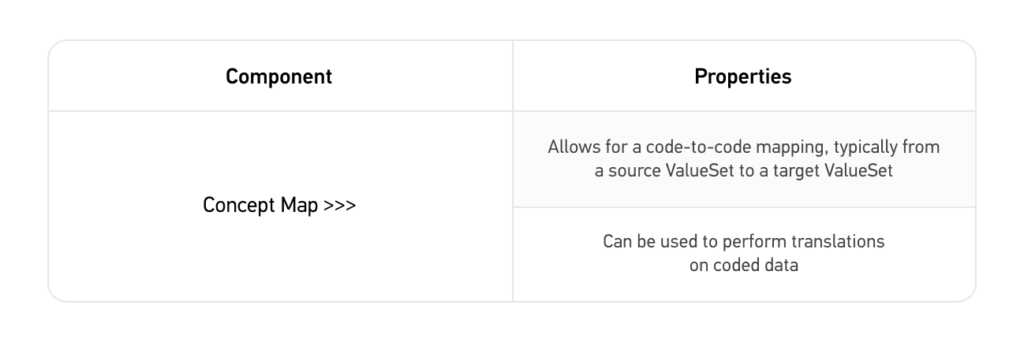
Concept map
A concept map is a mapping between two or more code systems or value sets. This allows healthcare providers to translate information from one code system to another, making it easier to communicate and share data across different healthcare systems. For example, a concept map might provide a way to translate codes from SNOMED CT to ICD-10, allowing healthcare providers to use the terminology most familiar to them.
ConceptMap operations
$translate
The $translate operation provides a way to map a code from one code system to a code in another code system.
Benefits of the FHIR Terminology Module
The healthcare industry relies heavily on accurate and comprehensive communication to ensure patients receive the best possible care. Using standardized terminologies can be a game-changer in this regard, enabling healthcare providers to communicate more effectively and efficiently.
- Improved interoperability and communication between different systems and applications.
- Reduced risk of miscommunication and errors in clinical decision-making.
- More efficient access to information, supporting high-quality, patient-centered care.
- Supports standardized code systems, value sets, and maps to ensure consistency and accuracy in clinical representation.
- Enables real-time clinical decision support and alerts to help prevent medication errors and adverse events.
- Improves care coordination and supports high-quality, patient-centered care.
Conclusion
We hope that this introduction to the terminology module of FHIR gave you the important information you were looking for. Because this module plays a crucial role in enabling healthcare providers to represent real-time patient data using standardized terminologies, while also ensuring seamless interoperability with other systems.
If you’re interested in learning more about how to work with the FHIR Terminology Server, check out our more technical guide on how to work with Сoded data types, Code Systems, and Value Sets in FHIR.
As part of our Kodjin Interoperability Suite, our team has developed our own Kodjin Terminology Service, which enables the connection and management of terminology systems of any size or complexity. It offers instant FHIR compatibility, strong performance, and exceptional flexibility, all in one package.
The Kodjin Terminology Server allows you to update terminologies on the fly and provides seamless integration with multiple standardized terminologies in healthcare, such as ICD-10, LOINC, SNOMED, and RxNorm as well as other proprietary code systems. Contact us to request a demo of our solutions that help bolster interoperability in a cost-saving and efficient manner!
FAQ
- How can healthcare professionals and developers get started with a FHIR Terminology Module?
Understanding the FHIR Terminology Module is key to leveraging FHIR’s full potential. For those seeking a deeper exploration of FHIR, the Ultimate Guide – What is FHIR offers a complete overview of this essential standard.
If you want to get started with a FHIR Terminology Module, you should first get acquainted with the FHIR specification and how the Terminology Module fits into the ecosystem. This article is a good place to start for healthcare professionals. Next you should identify which specific terminologies (e.g., SNOMED, ICD, etc.) are critical for your healthcare operations. Find a FHIR solution, such as the Kodjin FHIR Server that also comes with a Terminology Module, which support the required terminologies and contact the developers for consultation on how to best implement a FHIR server for your project.
For developers, a good place to start would be the FHIR specification. We also have a guide on managing a FHIR terminology module in our documentation.
- Can FHIR Terminology Module be used in conjunction with other healthcare standards?
FHIR Terminology Module is part of the FHIR specification, as such you can only use it with a FHIR Server. If you want to use FHIR in conjunction with other healthcare standards, there are various options that make it possible such as implementing an ETL process.