Your revenue cycle management (RCM) team resolves denied claims, improves front-end edits, and appeals claims faster each quarter. So why does the overall denial rate barely move? Why do the same payers, procedures, and departments keep generating the same problems?
Denial management analytics helps healthcare organizations reduce avoidable revenue loss. The real challenge, however, is understanding why denial risk keeps building upstream, in clinical workflows, documentation habits, and care variation, where the RCM team has limited direct influence.
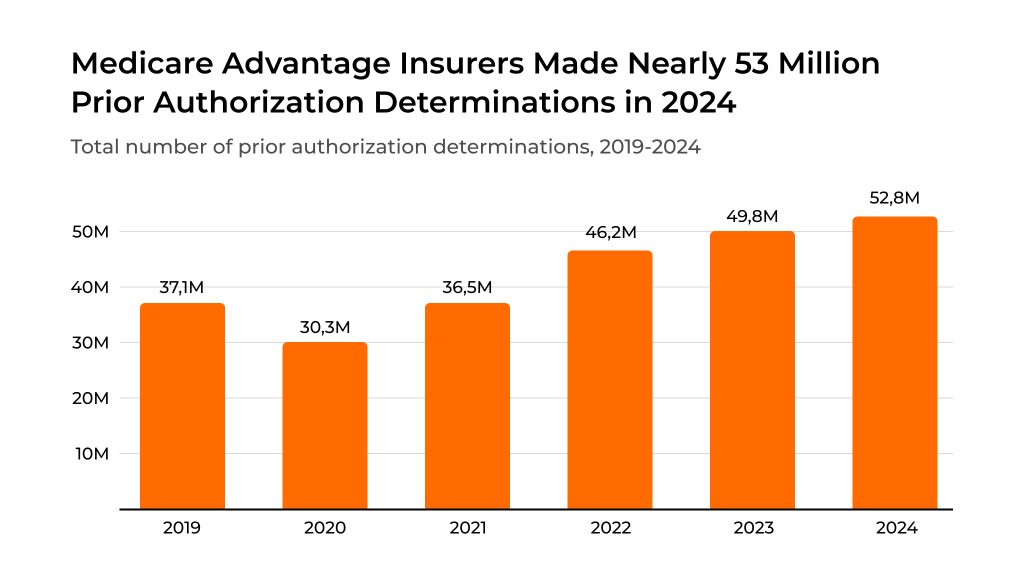
The scale of the problem is significant. According to the American Hospital Association (AHA), hospitals spent $43 billion in 2025 on collecting payments from insurers for care already delivered, including nearly $18 billion spent specifically on overturning claims denials alone. Medicare Advantage plans alone issued nearly 50 million prior authorizations (PAs) that same year. Much of this cost comes from re-solving problems whose root causes sit in clinical processes, far from the billing queue.
That is why traditional denial management often feels reactive and expensive. Teams see the problem only after the claim is denied, then correct, resubmit, or appeal. A broader analytical approach helps leaders identify recurring patterns across providers, departments, workflows, and patient groups, and trace them back to clinical decisions that drive denial risk. Kodjin supports this kind of work as a healthcare analytics platform built on connected clinical, operational, and financial data.
This article is written for Revenue Cycle Managers, RCM Directors, Healthcare CFOs, Clinical Department Heads, CIOs, and Operations Leaders. You will see where traditional denial analysis helps, where it plateaus, and how a broader view that connects clinical and financial signals changes who can act on denial risk and how fast they can respond.
Highlights
- The American Hospital Association (AHA) says hospitals spent $43 billion in 2025 on collecting payments from insurers for care already delivered, with nearly $18 billion spent specifically on overturning claims denials alone.
- Many recurring denials start with prior authorization timing, documentation quality, care variation, and fragmented workflows.
- The Healthcare Financial Management Association (HFMA) recommends tracking multiple denial metrics. Those include initial denial rate, denial write-offs, time to appeal, time to resolution, and the percentage of initial denials overturned.
- Kodjin fits best as a broader analytics layer that helps teams explore patterns across connected clinical, financial, and operational data.
Why Traditional Hospital Denial Management Fails Healthcare Organizations
Traditional denial programs focus on the moment the problem becomes visible: the denied claim. The team checks the denial code, reviews the payer response, corrects the issue, resubmits, or appeals. Over time, teams get faster at this cycle. But faster corrections do not reduce the volume of denials.
One core limitation is that the analysis remains focused on the claim itself and the bureaucratic procedures surrounding it. Everything the team examines, including denial codes, payer rules, submission errors, and appeal timelines, reflects the RCM team’s own activity. Meanwhile, a significant share of denials in healthcare originates in clinical decisions that happen before a claim is ever created.
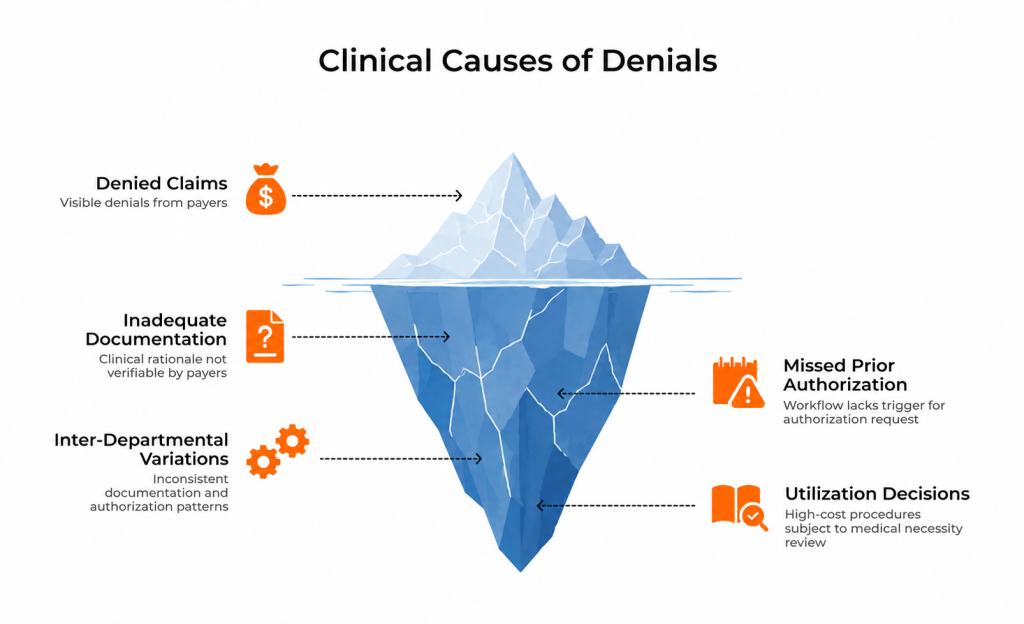
Consider the clinical causes that traditional denial analytics rarely surface:
- A treatment plan where the care was appropriate, but the clinical rationale was documented in a way the payer could not verify against their medical necessity criteria.
- A prior authorization was requested too late or missed entirely because the clinical workflow lacked a trigger point for it.
- Variation between departments or providers: one team documents and authorizes in a way payers accept, while another follows a different pattern and faces repeated pushback.
- High-cost procedures or extended lengths of stay that keep landing in medical necessity review, generating denials that trace back to utilization decisions, not billing mistakes.
These are systemic patterns rooted in how care is delivered, documented, and coordinated. They directly affect hospital claim denials and revenue cycle denial management KPIs, even though the RCM team can influence them only indirectly.
The challenge grows further because addressing clinical root causes is slow. Identifying a systemic issue at the clinical level, communicating it to the relevant department, reaching consensus on a workflow change, and measuring whether the change reduced denials can take 6 to 8 months.
The analysis itself is statistical: it requires patterns across encounters, providers, and time periods. You cannot easily isolate a single doctor, a single patient, or a single cohort.
Fragmented data makes the picture even harder to assemble. Signals are spread across electronic health records, claims systems, billing tools, payer portals, clearinghouses, and remittance files. Without a consistent data layer, teams end up with partial views that show what happened to the claim but reveal little about why the same problem keeps forming.
The financial impact is direct. Denials delay reimbursement, increase labor costs, slow cash flow, and create rework, even for claims that are eventually paid. When the same issue keeps appearing, the cost includes the appeal itself and the opportunity cost of an entire organization re-solving a problem that was never fixed at the source.
How Denial Management Analytics Works?
Denial management analytics brings together data from multiple sources to help organizations understand where denials occur, why they recur, and which workflows need earlier attention. The scope and depth of that analysis vary significantly depending on the approach.
Classic denial analytics: transaction-level focus
A traditional denial analytics setup works at the transaction level. It ingests claims, remittance data, payer responses, and denial codes. From there, it supports tracking initial denial rates, monitoring denial write-offs, measuring time to appeal and resolution, and identifying the percentage of denials overturned.
▶ The HFMA’s denial framework captures this well. It recommends tracking measures like initial denial rate, denial write-offs, appeal timelines, resolution speed, and overturn rates.
At the operational level, these tools can score claims for risk before submission, catch missing or incorrect data, and help teams decide where to focus based on payer-specific trends. Most also support a denial management process flow chart showing how a claim travels from submission through denial, correction, and appeal.
The limitation, however, is clear: classic analytics answers what happened to the claim and how the RCM team should respond. It does less well at answering why the same patterns keep forming upstream.
Broader analytics: connecting clinical and financial signals
A broader approach to medical claims denial management connects clinical, operational, and financial data into a single analytical layer. Instead of examining denials as billing events, it reconstructs the context in which claims are created: the patient journey, treatment decisions, documentation quality, authorization timing, and care variation across providers.
This is where Kodjin fits. Kodjin does not replace a denial scoring tool. It works at a different level, reconstructing the broader environment around denial risk, so teams can examine patterns that remain invisible in a transaction-centered view. With a healthcare data analytics solution like Kodjin, the question shifts from “Can we catch this claim before it fails?” to “Why are we generating this kind of claim in the first place?”
That distinction matters because it changes who can act. When the analysis stays at the claim level, the RCM team sees it and responds. When the analysis surfaces clinical and operational patterns, clinical department heads, operations leaders, and C-level executives get involved, and the response shifts from rework to prevention.
Key Use Cases of Broader Denial Management Analytics
The most useful denial analytics use cases help organizations reduce avoidable rework and act earlier, before recurring problems become a larger financial burden.
Predicting claim denials before submission
A denial analytics system reviews a claim before submission and estimates the likelihood of denial by comparing it to historical outcomes. This helps RCM teams focus on the claims most likely to fail, improving front-end review efficiency and reducing preventable denials.
With a broader platform like Kodjin, the question goes further: why is this type of claim being generated repeatedly? Are there clinical workflows, documentation practices, or authorization gaps that consistently result in high-risk claims? Using a claim denial rate benchmark, teams can compare performance across departments and track whether upstream interventions actually reduce denial volume over time.
Identifying root causes of denials
Classic tools identify the denial code and the payer’s stated reason. Kodjin helps teams go deeper: is the root cause a coding error, an eligibility gap, or an authorization process that consistently breaks down for certain procedures or facilities? Effective claims denial management includes the following: linking clinical encounter data to claims outcomes, enabling organizations to move beyond surface-level categorization to actionable root-cause analysis.
Payer behavior analysis
Denial patterns vary by payer. Some payers deny at higher rates for specific procedure codes, patient populations, or facilities. Analytics that track these patterns over time give organizations leverage in contract negotiations and help prioritize which payer relationships need strategic attention. This is a practical component of revenue cycle denials management that delivers measurable results.
Provider performance optimization
Denial pressure is rarely spread evenly. Some providers, departments, or facilities consistently generate cleaner claims and face fewer reimbursement issues. Others show recurring patterns linked to documentation, timing of authorization, or care variation.
Classic analytics can show that one department has a higher denial rate. Kodjin helps examine the larger pattern: is it a documentation habit, a workflow gap, or a care variation issue? That turns benchmarking into a practical tool for targeted training, workflow redesign, and cross-departmental alignment, supporting effective hospital denial management by connecting clinical behavior to financial outcomes.
How Kodjin Analytics Enables Predictive Denial Management
Kodjin Analytics supports predictive denial management beyond scoring a single claim before submission. Kodjin works earlier by reconstructing the clinical, operational, and financial context in which claims are created, enabling the identification of systemic risk before it reaches the billing queue.
The key difference: classic denial analytics helps RCM teams react faster. Kodjin helps clinical department heads, RCM directors, and C-level leaders understand where denial risk is forming and intervene at the source.
▶ Classic denial analytics operates at the transaction administration level. Kodjin works at the strategic analysis and prevention levels. The first tells you what went wrong with a claim. The second tells you why your organization keeps producing that kind of claim.
Unified healthcare data layer
Kodjin brings together fragmented clinical, operational, and financial data into one consistent analytical layer. Denial risk rarely resides in a single system. It forms across encounters, orders, authorizations, billing records, and payer interactions. With that broader context, teams move past flat denial summaries into the conditions surrounding recurring reimbursement issues.
Real-time denial insights and dashboards
Kodjin gives teams a way to explore denial-related patterns as they emerge, through interactive, conversational exploration of data rather than fixed dashboard views. If denials rise in one service area, a department head can explore whether the increase correlates with certain facilities, procedures, patient groups, or workflow steps, and respond before the pattern becomes entrenched.
Longitudinal pattern analysis and risk scoring
Querying Kodjin’s analytical layer reveals patterns invisible in monthly reports: cost concentration across patient cohorts, care variation between providers, and the relationship between clinical decisions and payer outcomes over time. This supports predictive risk scoring that extends beyond individual claims to systemic behavior, helping organizations set and track a meaningful benchmark for claim denial rates.
Root cause analysis and drill-down capabilities
If repeated denials are linked to missing prior authorization, a classic tool responds with another front-end check. Kodjin helps teams step back and ask: where does the authorization process break down? Is it specific to certain facilities, procedures, or payer contracts? The same logic applies to duplicate services, extended stays, or procedures that repeatedly trigger payer pushback. Instead of fixing one claim at a time, teams identify the operational and clinical patterns that create the problem. This aligns with a behavioral data analytics approach to understanding why processes fail.

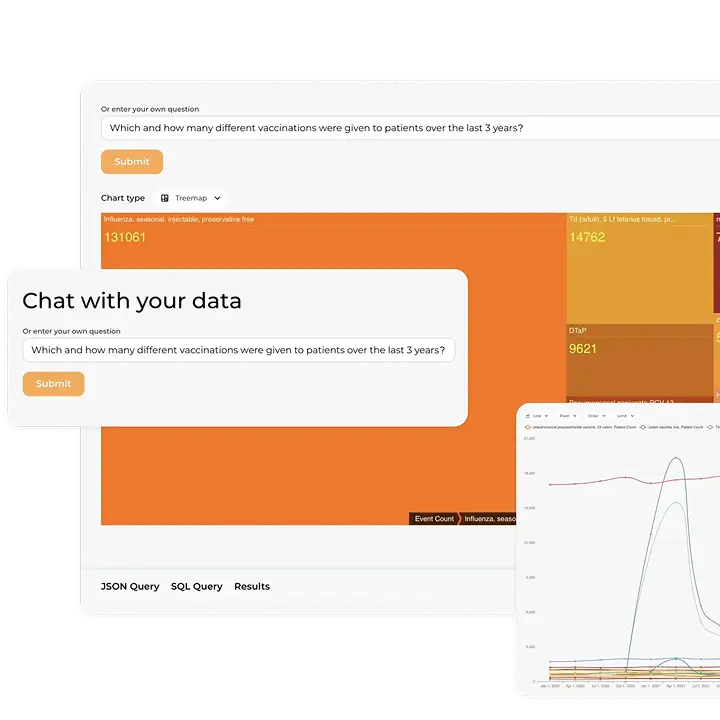
Conversational AI interface for non-technical users
One of the more practical things about Kodjin is that you don’t need SQL skills or a data team to get answers. The platform offers a conversational AI interface: users can ask questions in plain language, like “Which departments had the highest denial rates for Medicare Advantage last quarter?” or “What changed in prior auth timing for cardiology over the past six months?”.
The conversational AI interface opens denial analytics to the people closest to the problem: clinical leaders, department heads, and operations managers who know their workflows but may never have had direct access to this kind of data.
Scalable and customizable architecture
Kodjin supports evolving questions across the revenue cycle, operations, and care delivery. Payer behavior changes, internal workflows change, and operational priorities shift. Teams need a platform that grows from monitoring denials into optimizing clinical-financial alignment across the organization. For more on how analytics supports the broader claims management process flow, see our detailed guide.
Conclusion
The most valuable use of denial management analytics is helping organizations not only understand why denial risk keeps forming across clinical workflows, documentation habits, utilization patterns, and fragmented data, but also predict where new risks are likely to emerge before they reach the billing queue. That predictive capability shifts the focus from reactive correction to earlier, more strategic prevention — and puts that insight into the hands of the people who can change it.
Traditional denial tools still matter. They support correction, appeals, and short-term recovery. But organizations that want to move their overall denial rate need a broader perspective. They need to connect clinical behavior to financial outcomes, surface systemic patterns, and bring clinical department heads and C-level leaders into the conversation.
That is where Kodjin stands apart. As a conversational, self-service analytics platform built on connected healthcare data, Kodjin provides a single, coherent view of the clinical and financial signals that drive denial risk. The result: both clinical and financial teams work toward the same goal, improving the efficiency and sustainability of the entire organization.
Explore our Conversational Healthcare Software
Learn more
FAQs
What data is needed to start with denial management analytics?
At a minimum, organizations need claims, remits, denial reasons, payer data, and core workflow timestamps. For a more preventive model, they also need upstream context such as encounters, orders, provider data, authorization events, and documentation signals.
How is Kodjin different from a denial prediction tool?
A denial prediction tool usually scores claims close to submission. Kodjin is better suited for broader analysis. It helps teams examine patient journeys, provider variation, utilization patterns, and workflow breakdowns that increase the likelihood of denials upstream. Kodjin’s public analytics page describes this through conversational access, a semantic layer, and shared business concepts across fragmented healthcare data.
Can this approach work for hospital denial management programs?
Yes. Hospitals often see the greatest value from this approach because denials frequently involve complex pathways, multiple handoffs, prior authorization, necessity reviews, and variation across departments.
How long does it take to see value from medical claims denial management analytics?
Traditional denial reporting can show patterns fairly quickly once the data is organized. Strategic prevention takes longer because it depends on workflow changes, documentation improvements, or changes in provider behavior. The first gains usually come from better segmentation and faster root-cause visibility. The larger gains come when operational and clinical owners begin acting on the same signals rather than treating denials as a finance-only problem.
What happens if organizations keep treating denials only as a back-end revenue cycle issue?
They may still recover some revenue, but they also keep reproducing the same causes. That leads to more rework, slower cash flow, more administrative burden, and limited movement in overall denial performance. The fact that so many denied claims are eventually paid after repeated review is a strong sign that many organizations are still spending too much energy downstream.