Clinical trial analytics helps research teams use clinical, operational, and real-world data to make better decisions across the trial lifecycle. It is not just a dashboard after data lock. At its best, it becomes a real-time analytics layer that delivers on-demand, actionable insights when they matter most — supporting feasibility, patient recruitment, trial monitoring, safety analysis, and evidence generation.

Clinical trials already produce and depend on large amounts of data: EHR records, lab results, claims, registries, EDC systems, patient-reported outcomes, and post-market data. The issue is not that data does not exist. The issue is that it is often fragmented, inconsistently coded, and difficult to use when trial teams need answers.
That is where analytics in clinical trials becomes strategic. It helps organizations move from scattered information to governed, research-ready intelligence.
Explore our Advanced Healthcare Analytics Software
Learn more
Highlights
- Clinical trial data analytics supports feasibility, recruitment, monitoring, safety, and evidence generation.
- Recruitment delays are often not only outreach problems. They are data usability problems.
- FHIR® and OMOP can help connect clinical care data with research analytics.
- AI can support faster analysis, but only when it works with governed data and approved definitions.
- Kodjin Analytics by Edenlab helps turn fragmented healthcare data into queryable, decision-ready insights and dashboards for every role in an organization.
Why Is Clinical Trial Recruitment Still So Difficult?
Clinical trial recruitment is often treated as a patient outreach or engagement challenge. That is true, but only partly.
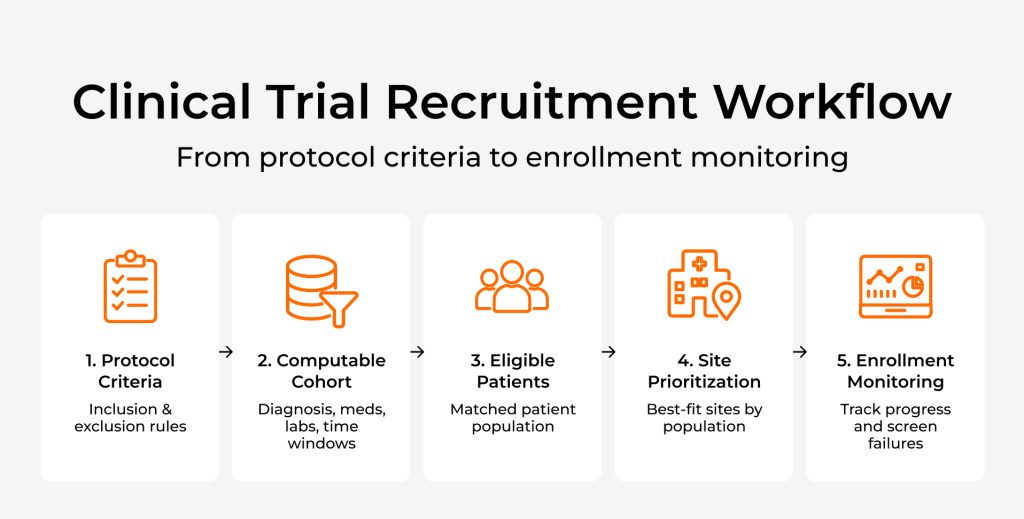
Before a study team can reach the right patients, it first needs to identify them reliably. That means translating protocol criteria into clinical logic that can be applied across EHRs, lab systems, claims, registries, and trial platforms.
This is where recruitment becomes a data infrastructure problem.
Eligibility criteria are rarely simple. A patient may need to match a diagnosis, medication history, lab result, prior procedure, treatment timeline, and exclusion rule at the same time. One condition may be stored in the EHR. Another may appear in claims data. A lab result may exist, but use a local code. A treatment history may be split across several systems.
As a result, a patient can look eligible in one dataset and ineligible in another. Sites may overestimate the available population. Research teams may spend time on manual pre-screening only to face high screen failure rates later.
This is why slow recruitment is not always a failure of effort. Often, it is a failure to turn fragmented clinical data into computable cohorts that trial teams can trust.
From Fragmented Data to Computable Cohorts
The central problem in clinical trial data management is not only data collection. It is making that data usable for clinical questions.
For example, a trial team may need to identify patients who have a specific diagnosis, received a certain treatment, have lab values within a defined range, have not received a conflicting therapy, and meet these conditions within a specific time period.
This is not a simple reporting query. It requires clinical context, terminology normalization, longitudinal data, and temporal logic. In practice, the question is not only “How many patients do we have?” but “How many patients meet this exact clinical definition, at the right point in their care journey, according to data we can trust?”
FHIR helps by giving healthcare systems a structured way to exchange clinical data. HL7 Vulcan’s Real World Data project, which aims to bridge routine patient care and clinical research, shows how FHIR can support research-relevant data retrieval from EHR systems. OMOP CDM also plays an important role by standardizing observational healthcare data for analysis across datasets and institutions.
But neither FHIR nor OMOP automatically makes data ready for trial decisions. Standards provide the foundation. Trial analytics still needs a semantic layer that defines clinical concepts, measures, cohorts, time windows, and outcomes in a consistent way.
This matters because trial teams often reuse the same concepts across studies: eligible patients, abnormal results, treatment delays, follow-up windows, safety events, and outcomes. If each team defines these concepts differently, analytics becomes difficult to compare, audit, or reuse.
Of course, for regulatory submission workflows, FHIR and OMOP do not replace CDISC standards such as SDTM and ADaM. Their value is mainly upstream: improving how clinical and real-world data is accessed, standardized, analyzed, and prepared for research use.
That is the difference between having data and having clinical data insights that a research team can actually trust.

How Clinical Trial Analytics Supports the Trial Lifecycle
The value of clinical trial analytics goes beyond recruitment. Once cohort logic, terminology, and longitudinal data are available in a governed analytics layer, the same foundation can support decisions across the entire trial lifecycle.
Feasibility and site selection. Research teams can estimate whether enough eligible patients exist, which sites have relevant patient populations, and whether protocol criteria are too restrictive.
Patient recruitment and enrollment. Teams can identify potential cohorts faster, understand why patients fail screening, and adjust recruitment strategies based on real data.
Trial monitoring and safety. Analytics can help track enrollment, protocol deviations, missing data, adverse events, and operational risks before they become larger problems.
Outcomes and evidence generation. After or alongside a trial, data can be used to understand treatment patterns, patient journeys, and real-world outcomes.
This is where clinical research analytics becomes more than operational reporting. It connects trial execution with evidence-based innovation by helping teams ask better questions, test assumptions, and turn clinical data into evidence that can support better research decisions.
Why AI Needs a Governed Data Foundation
There is a clear role for data science in clinical trials. AI and advanced analytics can help with cohort discovery, feasibility analysis, dropout risk prediction, anomaly detection, and natural-language querying. But in clinical research, faster answers are not enough. The answer also needs to be explainable, traceable, and based on approved definitions.
If AI identifies a potential cohort, the research team needs to know which criteria were used. If it flags a safety signal, users need to understand the source data and the logic behind the alert. If it answers a natural-language question, it should not invent joins, use unapproved formulas, or ignore governance rules.
This is why clinical development analytics cannot be separated from data governance. AI is only useful when it works inside a controlled analytics environment where access, definitions, terminology, and query logic can be reviewed.
For clinical trial and research use cases, this also means role-based access, auditability, and de-identification or pseudonymization where required. The goal is not to expose sensitive data to a model. The goal is to help users ask better questions against governed data.
The future is not “AI over messy data.” It is AI supported by standardized data, semantic definitions, and trusted analytics workflows.
How Kodjin Analytics Fits Into This Architecture
Kodjin Analytics supports this shift by helping healthcare and research organizations turn fragmented clinical data into governed, queryable intelligence. Its value is not limited to visualizing trial metrics after the fact. The stronger role is the analytics foundation underneath: the layer that connects data sources, standardizes clinical meaning, defines reusable measures, and makes complex healthcare data easier to explore on an on-demand basis.
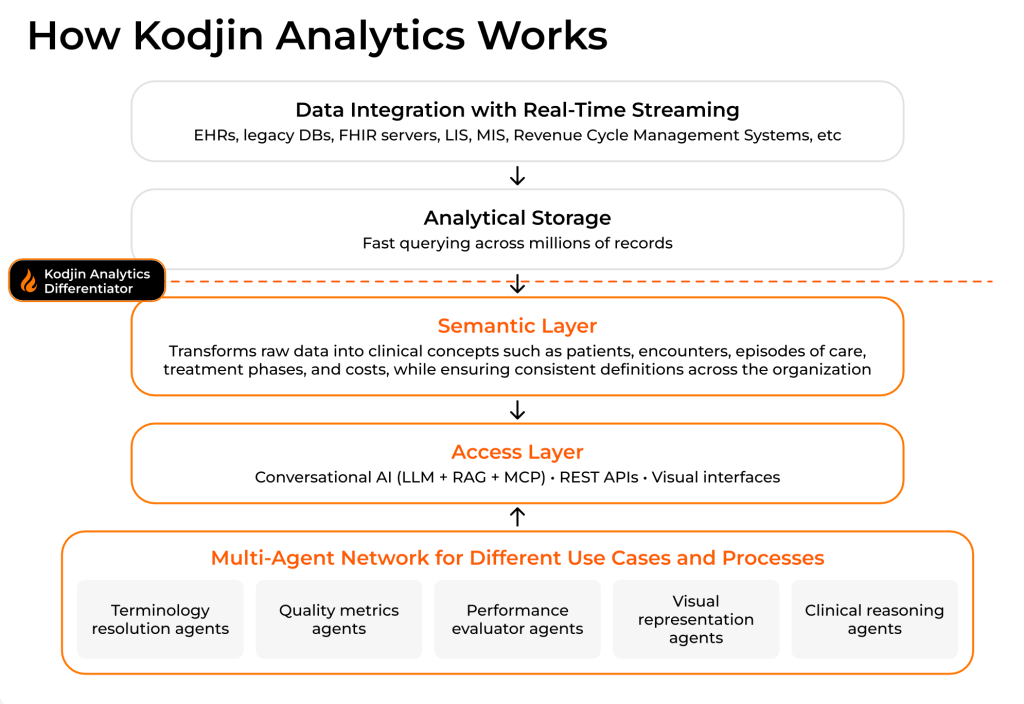
At the data foundation level, Kodjin Analytics can work with FHIR-based healthcare data pipelines and support data coming from EHRs, registries, labs, claims, and other clinical systems. For organizations using OMOP-based research environments, it can also support the broader goal of turning observational healthcare data into consistent analytical logic for cohort analysis, outcomes research, and real-world evidence workflows.
The key differentiator is the semantic layer. Instead of forcing every clinical or research question to become a custom SQL task, the semantic layer defines approved concepts, measures, dimensions, relationships, and time windows. For example, concepts such as “eligible oncology patients,” “abnormal lab result,” “treatment delay,” or “follow-up within 90 days” can be modeled once and reused across studies, dashboards, and analytical workflows.
This is also where AI becomes useful in a safer and more practical way. With natural-language analytics, users can ask questions in plain language, while the system translates those questions into structured queries against governed data models. The AI does not need to see raw patient data to generate query logic. It works with metadata, schema, and approved definitions, while the actual query execution remains inside the customer’s controlled environment.
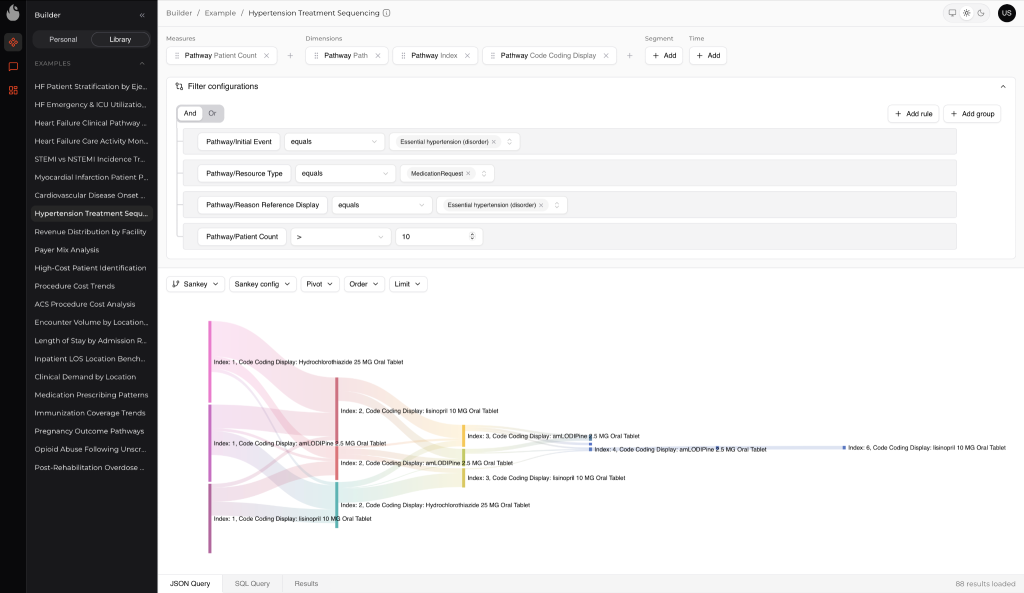
For example, a clinical research lead could ask: “Show patients over 60 with an abnormal lab result who did not receive a follow-up procedure within six months.” Kodjin Analytics can use the semantic layer to interpret the clinical concepts, apply the right time window, query standardized data, and return a cohort that can be reviewed, refined, and traced back to the underlying logic.
The impact extends across the entire clinical trial lifecycle. Whether teams are assessing study feasibility, identifying eligible participants, monitoring trial progress, or generating real-world evidence, success depends on having reliable access to clinically meaningful insights that can be explored quickly, understood clearly, and trusted by stakeholders.
Kodjin Analytics is not just another dashboard tool. It acts as an analytics foundation for cohort discovery, longitudinal analysis, pathway analysis, operational monitoring, and real-world evidence workflows. It helps clinical, operational, and research teams move faster without losing control over definitions, data access, or trust in the results.
Conclusion
Clinical trial analytics is not just a reporting function. It is becoming part of the operational backbone for modern clinical research. The trials that move faster will not simply be the ones with more data. They will be the ones that can turn data into trusted decisions: who to recruit, which sites to select, what risks to monitor, which outcomes matter, and how real-world evidence can support innovation after the trial ends.
The real shift is from fragmented tools to connected intelligence. Clinical research teams need data that is not only available, but standardized, explainable, governed, and ready for action.
FAQ
What is clinical trial analytics?
Clinical trial analytics is the use of clinical, operational, and real-world data to improve decisions across trial planning, recruitment, monitoring, safety, outcomes, and evidence generation.
How is clinical trial analytics different from BI dashboards?
Dashboards usually show what already happened. A stronger analytics layer helps teams ask deeper questions about cohorts, eligibility, site performance, risks, outcomes, and patient journeys.
Where do FHIR and OMOP fit?
FHIR helps exchange healthcare data in a structured way. OMOP helps standardize observational data for research and analysis. Both can support clinical trials data analytics, but they still need governance, terminology alignment, and semantic logic on top.
How does Kodjin Analytics support clinical trial teams?
Kodjin Analytics helps make healthcare data easier to query and interpret through semantic modeling, natural-language analytics, cohort discovery, longitudinal analysis, and governed access to clinical data.